
{kind=link}
Abstract
Citation: Kusuma D, Atanasova P, Pineda E, Anjana RM, De Silva L, Hanif AA, et al. (2022) Food environment and diabetes mellitus in South Asia: A geospatial analysis of health outcome data. PLoS Med 19(4):
e1003970.
https://doi.org/10.1371/journal.pmed.1003970
Academic Editor: Barry M. Popkin, Carolina Population Center, UNITED STATES
Received: October 17, 2021; Accepted: March 18, 2022; Published: April 26, 2022
Copyright: 2022 Kusuma et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The surveillance and the environmental data are available to researchers upon request to the study Data Access Committee. For the surveillance data, contact forms and emails are provided on the GHRU website (www.ghru-southasia.org). For the environmental data, requests should be made via email to [email protected].
Funding: This article was funded by the National Institute for Health Research (NIHR) (16/136/68) using UK aid from the UK Government to support global health research (JCC) and the LISS DTP funded by the Economic & Social Research Council (ESRC) (ES/P000703/1). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
Abbreviations:
AME,
average marginal effect; AOR,
adjusted odds ratio; FFR,
fast-food restaurant; FV,
fruits and vegetables; GDP,
gross domestic product; GHRU,
Global Health Research Unit; GIS,
geographic information system; LMIC,
low- and middle-income country; NCD,
noncommunicable disease; OLS,
ordinary least squares; OR,
odds ratio; PPP,
purchasing power parity; SES,
socioeconomic status; STROBE,
Strengthening the Reporting of Observational Studies in Epidemiology; T2DM,
type 2 diabetes mellitus
Introduction
With a global prevalence of 9% (463 million people) in 2019, the widespread epidemic of type 2 diabetes mellitus (T2DM) renders its prevention a major public health priority [1]. Although, historically, T2DM was considered a disease confined to countries of affluence, recent estimates suggest that 80% of the 463 million people with T2DM now live in low- and middle-income countries (LMICs) [2]. South Asia is particularly affected by T2DM, where the highest number of deaths were attributable to diabetes under the age of 60 years (working age) in 2019. The projected increase in T2DM prevalence for 2030 in the region is substantially higher (74%) in comparison to that in Europe (15%) [1].
In 2020, the Lancet Diabetes Commission recommended creating health-enabling environments that promote healthy eating and physical activity to reduce the number of people suffering from T2DM [3]. This highlights the importance of the role the food environment plays in driving diabetes prevalence. A cohort study of the United Kingdom Biobank using a sample of 502,625 participants found that the density of ready-to-eat food establishments (pubs and bars, restaurants and cafeterias, and fast food or hot and cold takeaway outlets) within a 1-km street catchment area was associated with higher odds of T2DM [4]. Another cohort study of more than 4.5 million participants from Sweden found that the density of health-harming food outlets (fast-food outlets, convenience stores, bars, and pubs) within 1-km buffer from an individuals home was associated with a greater likelihood of T2DM prevalence and incidence [5]. Moreover, den Braver and colleagues conducted a systematic review of 109 eligible studies and found that living in an urban residence was associated with higher T2DM risk. However, it found that evidence of an association between food environment with T2DM risk remains inconsistent [6].
In this study, we assessed the role food environment plays on diabetes outcomes among adults in 2 understudied LMICs, Bangladesh and Sri Lanka, where the prevalence of diabetes has been growing rapidly. In 2020, the prevalence of diabetes was 8.1% and 8.7% in Bangladesh and Sri Lanka, which correspond to, respectively, an estimated 8.4 million and 1.2 million total cases of diabetes among adults [7]. These trends may be driven by an increase in the prevalence of risk factors for diabetes such as obesity and poor diets. The prevalence of obesity was 25.9% in 2018 and 29.3% in 2014 among adults in Bangladesh and Sri Lanka, respectively [8]. Moreover, evidence from Sri Lanka indicates that in 2013 only 3.5% of adults consumed the recommended 5 portions of fruits and vegetables (FV). In contrast, they consumed over 14 portions of starch and 3.5 portions of added sugars daily [9]. Further, consumption patterns and food sourcing have been found to vary across sex and the different income strata. For example, higher-income individuals are more likely to source food from conveniently located stores that might offer more product variety at higher prices, whereas lower-income groups are more likely to travel longer distances to stationary and/or mobile markets where the food is relatively cheap and readily available [10]. Food environments have been found to influence diets and obesity and therefore may be instrumental for the prevention of diabetes in these countries [3,11,12]. Yet, evidence on the association of the food environment and diabetes is limited, and, to our knowledge, no study has assessed this association in South Asia.
Most existing evidence is for high-income countries (e.g., United States, United Kingdom, Australia, Japan, and Sweden) and measure exposure to food environments using geographic information systems (GISs) data of food environments (e.g., density or proximity of food outlets) [6]. There are some contributions in LMICs (e.g., Thailand, Malaysia, India, Sri Lanka, Ghana, Nigeria, and Uganda), but exposure to food environments tends to be captured with crude metrics such as residency in urban/rural areas, which are imperfect in capturing the different elements of the environment as well as individual exposure to those environments. Second, previous studies focused on self-reported diagnosed T2DM status, which may have been subject to recall bias and did not included the undiagnosed populations, as shown by the UK Biobank study [4]. Thus, our study aims to fill the evidence gap by investigating the associations between the density and proximity of food environment and T2DM in Bangladesh and Sri Lanka, using a rich characterization of exposure to healthy and unhealthy food environments in the neighborhood of peoples homes. Our research question is whether food environment is associated with T2DM. We hypothesize that healthy elements of the food environments are negatively associated with T2DM, while unhealthy elements of the food environment are positively associated with T2DM.
Methods
South asia biobank
The South Asia Biobank is a comprehensive biobank of South Asian individuals, established to identify the risk factors and their complex interactions underlying the development of T2DM, cardiovascular disease, and other chronic diseases in South Asians. It is a cross-sectional investigation in Bangladesh, India, Pakistan, and Sri Lanka with data collected between November 2018 and March 2020. Data include participants demographic, lifestyle, clinical, environmental, and phenotypic characteristics and biological samples. In each country, national administrative data were used to select rural and urban surveillance sites. One district was randomly selected from each of the major administrative divisions or provinces, from which one subdistrict was randomly chosen. One or more community clinics (or urban dispensary) within each subdistrict were randomly selected and the ward where those community clinics located were surveillance sites. All eligible residents in a surveillance site were invited to participate. In the recruitment of participants, governmental census data and available household listings were used, together with house-to-house visits by local research teams, to identify the residents. Further detail on the sample and data can be found in Song and colleagues [13].
Outcome variables
There were 3 outcome variables in our analyses: diagnosed diabetes, fasting blood glucose level, and high blood glucose. First, diagnosed diabetes was a binary variable with a value of 1 if one reported ever been told by health worker having a raised blood sugar (i.e., diabetes) or currently takes medications (e.g., insulin) and 0 if otherwise. An interviewer-administered health and lifestyle questionnaire was used to collect information on diagnosed diabetes, along with other behavioral risk factors (smoking, alcohol use, physical activity, and consumption of FV), medical history, medications, and socioeconomic status (SES). Although diagnosed diabetes was self-reported, individuals were asked whether they had been told by their doctor they had diabetes or if they were on prescribed medication (e.g., insulin) rather than whether they thought they had diabetes. This, together with the fact that data collection took place in a healthcare setting, may mitigate some of the issues associated with self-reported data. However, to mitigate biases from self-reported data, we complement the analyses with 2 objectively measured outcomes, namely fasting blood glucose level (mg/dl), which was a continuous variable obtained from blood samples taken by trained data collectors in each surveillance site in the South Asia Biobank study and high blood glucose, which was a binary variable with a value of 1 if the fasting blood glucose was 126 mg/dl and above and 0 if otherwise. Fasting glucose was measured by point of care tests. Equipment, protocols, and training were standardized across surveillance sites [13].
Environmental mapping
In each surveillance site in Bangladesh and Sri Lanka, an environmental mapping was conducted to characterize the built environment in terms of the number of food outlets. We created a list of questions including geolocations, type of food outlets, and select items sold (e.g., FV, confectionary, and fast food). To ensure comprehensiveness, we adapted the questions and data collection procedure from the International Network for Food and Obesity/NCDs Research, Monitoring and Action Support (www.informas.org) and Johns Hopkins Universitys Maryland Food Systems Map (https://mdfoodsystemmap.org). We then discussed with local research teams to include local-specific food retailer types and food items sold. We included all questions in an online questionnaire using KoBoToolbox application (www.kobotoolbox.org) as the study instrument. Prior to data collection, local research teams in each country were trained in administering the instrument on smartphones or tablets. During October 2018 to August 2020, 6-person research teams conducted ground truth data collection surveys, by systematically covering all streets within surveillance sites on foot, following a map in which the site boundary was previously defined [13]. The team examined and recorded the presence of any food retailer within each site. To ensure that all streets and neighborhoods in surveillance sites were covered, we reviewed the map of food outlets on KoBoToolbox website and Google Maps together with each country team. Also, we deployed quality control checks by sending a second team to the sites to conduct spot checks in randomly selected areas within each site to ensure that all areas were appropriately covered and all relevant food outlets were recorded [14]. Our mapping collected data on geolocations (latitude and longitude) of supermarkets, corner stores (including small grocery and convenient stores), mobile food carts, stationary food carts, and restaurants. Mobile food outlets (stalls, carts, vans, and bikes) are important source of both healthy (e.g., fish and FV) and unhealthy food (e.g., snacks and sugary drinks) especially in LMICssample images from our mapping are in S1 Fig. Therefore, it was important to capture their availability. Because they are mobile, teams would visit the sites both in the mornings and afternoons, and control checks were performed in days and times that differed from the original data collection timings to ensure the presence of these outlets would be captured in the data.
Food environment exposures
To our knowledge, there is no food outlet classification in South Asia, and, therefore, we followed the international classification of healthy and unhealthy food outlets as described in the Retail Food Environment Index [15] and the North American Industry Classification System (www.census.gov/naics). We created 5 categories for food outlets: (1) fast-food restaurants, including international as well as domestic fast-food restaurants where people can purchase sweetened beverages and speedy, ready-to-eat food that is highly processed and high in calories and thus considered unhealthy; (2) supermarkets, self-service shop selling fresh FV and other healthy foods, therefore considered healthy; (3) corner stores, small shop selling foods; (4) mobile carts, temporary structure that is readily moveable; and (5) stationary carts, moveable structure but occupies a specific location [16,17]. Since we did not observe what is sold in each outlet, in reporting the results, we followed the literature in classifying supermarkets as healthy food outlets and fast-food restaurants as unhealthy food outlets [17]. Even though supermarkets sell a range of healthy and unhealthy products, in international classifications, these are described as healthy due to the fact that they are more likely to provide healthier options compared to fast-food restaurants (FFRs) or corner stores [15]. Therefore, for supermarkets and FFRs, we adopt the terminology of healthy and unhealthy food outlets as in international classifications for the purpose of formulating our research hypotheses, but we remain agnostic to the direction of the association of each food retailer on diabetes outcomes [15]. For stationary carts and mobile carts, there is no consensus in the literature on their classification, and, therefore, we remain agnostic, in terms of research hypotheses, on whether they are healthy or unhealthy.
We calculated the density of and proximity to fast-food outlets, supermarkets, corner stores, mobile carts, and stationary carts, which together encompasses what we here refer to as the food environment. Food environment geolocation data were merged with individual-level data to characterize the density of different food outlet types within 300-m buffer around each participants home. We counted the total number of each food outlet and defined density as the share of each food outlet type relative to all food outlets within the 300-m buffer. Also, we defined the proximity of food outlets as having at least 1 food outlet type within 100-m of a participants home addressvariable definitions are summarized in S1 Table. Similar distances have been used in the literature and enables capturing more variation in terms of individual exposure to the food environments [18,19]. Geospatial analyses were conducted on ArcMap 10.3.
Data analysis
For fasting blood glucose level (a continuous variable), we employed ordinary least squares (OLS) multivariate regressions to assess its association with food environment. In reporting the estimates, we used the OLS coefficients for both density and proximity as the measure of food environment exposure. For high blood glucose and diagnosed diabetes (binary variables), we employed logistic regressions to test the associations with food environment. In reporting the estimates, we report average marginal effects (AMEs) for density (a continuous variable) and adjusted odds ratios (AOR) for proximity (a binary variable), as the measures of food environment exposure. In addition to these models using the entire sample, we also stratify by sex and income. The low- and high-income strata were defined based on whether each individual had an income of above (henceforth high income) or below (henceforth low income) the median income among the sample in each country.
We adjusted for individual-level covariates based on previous literature [20]. They included demographic characteristics (i.e., sex, age, country, marital status, and religion), SES (i.e., paid employment, school years, income, and household composition), health status measured (i.e., self-assessed health), healthcare utilization (i.e., receiving advice from health workers to reduce the consumption of products high in fat and sugary beverages, to increase daily intake of FV, to lose weight, or to increase physical activity), and physical activity habits (i.e., weekly minutes of vigorous or moderate physical activity spent at work, home or recreational facilities, and walking or cycling as a mode of transportation). We control for religion because, in the context of South Asia, studies have reported that religious affiliations could significantly impact individuals dietary patterns, physical activity, and, ultimately, may impact the risk of diabetes and other noncommunicable diseases (NCDs). For example, evidence suggests that Muslim populations tend to have higher prevalence of NCDs and indicated that Muslims consume more deep-fried and processed foods and spend less time in physical activity (especially Muslim women) compared to non-Muslim, even when controlled for education and income status [21].
Income was reported in USD after being adjusted for purchasing power parity (PPP) for comparability between the 2 countries and was deflated using 2018 prices. Regressions also included surveillance site as the fixed effects to control for site-specific time invariant cofounders. The analyses were well powered using a sample of 12,167 participants and conducted in STATA 15.1. More details of model specifications are provided in S1 Text, and estimates from unadjusted regressions are provided in S2 Table. This study is reported as per the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelinesee provided in S3 Table.
The study did not have a published protocol, but it had a planned analysis in the research proposal and research plans submitted to the funder (S2 Text). Also, the study had a (nonwritten) internal plan for the analyses, which were assessed by the Global Health Research Unit (GHRU) Steering Committee. We have not deviated from the planned analyses during the execution of the analyses, nor during the review process.
Research approval was obtained from the Imperial College London Research Ethics Committee (reference: 18IC4698) and local institutional review boards in each of the participating countries (Bangladesh [BRAC University] and Sri Lanka [University of Kelaniya and University of Colombo]).
Results
For the total sample of N = 12,167, which included participants from Bangladesh (N = 8,534) and Sri Lanka (N = 3,633), the average age was 45.5 (14.4 SD) years, school years were 6.42 (4.84 SD), and monthly income was 700.73 USD (Table 1). From the total, 59.7% (49.1 SD) were females, and 43.9% had a paid employment. Regarding the food environment (panels B and C), the average share of FFR within 300 m of a residents home address was 7.78% (9.74% SD). Corner stores and supermarket shares were 50.79% (33.20% SD) and 0.88% (3.37% SD), respectively. The share of FFR was higher in Bangladesh, while the share of corner stores and supermarkets were higher in Sri Lanka. The share of supermarkets was zero in rural areas, indicating that all supermarkets in our sample were in urban sites. For diabetes mellitus, defined as high blood glucose (>126 mg/dl) and diagnosed diabetes, the mean fasting blood glucose level was 102.92 (33.86 SD) mg/dl. The proportion of high blood glucose (>126 mg/dl) was 11.13% (31.46% SD) and that of diagnosed diabetes was 11.90% (32.39% SD). Diabetes mellitus levels were higher among females and higher-income participants (Table 1).
Regarding the associations between fasting blood glucose level and the density and proximity of food outlets, no statistically significant results were found for the share of supermarket, corner stores, stationary carts, or mobile carts (Fig 1, Tables 2 and 3). However, a higher FFR share was associated with a 9.21 mg/dl blood glucose increase (95% CI, 0.17, 18.24; p < 0.05). Similarly, having at least 1 FFR in the proximity (i.e., within 100 m) of ones home was associated with 2.14 mg/dl blood glucose increase (CI: 0.55, 3.72; p < 0.01). When stratifying by sex, FFR densities/shares were associated with a greater blood glucose increase in females ( = 13.37; CI: 0.59, 26.16; p < 0.05), while FFR proximities were associated with a higher blood glucose increase in males ( = 3.15; CI: 0.39, 5.91; p < 0.05) and in those with higher income ( = 3.84; CI: 0.68, 7.00; p < 0.05).
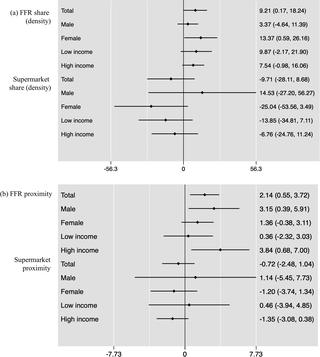
Fig 1. Associations between fasting blood glucose level and density (a) and proximity (b) of food outlets.
Note: The values show OLS regression coefficients; 95% CIs in brackets. Density = the number of each food outlet per total number of food outlets within 300 m of a residents home address. Proximity = 1 if having at least 1 outlet within 100 m of a residents home address and 0 if otherwise. FFR, fast-food restaurant; OLS, ordinary least squares.
Fig 2 shows the associations between the density of food outlets and diabetes mellitus (Tables 2 and 3). Overall, no statistically significant results were found for the share of supermarket, corner stores, stationary carts, and mobile carts (Table 2, panels B and C). However, results showed that the density/share of FFR in the neighborhood of individuals homes was positively associated with the probability of being diagnosed with diabetes. A 1% increase in the share of FFR near an individuals home was associated with 8% increase in the probability of being clinically diagnosed as a diabetic (AME: 0.08; CI: 0.02, 0.14; p < 0.05). When stratifying by sex, while stronger among females (AME: 0.10; CI: 0.01, 0.18; p < 0.05) and higher-income populations (AME: 0.09; CI: 0.01, 0.17; p < 0.05), these associations were also statistically significant in males (AME: 0.06; CI: 0.001, 0.12; p < 0.05) and lower-income populations (AME: 0.07; CI: 0.001, 0.13; p < 0.05).
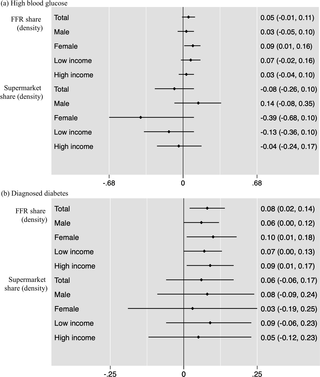
Fig 2. AMEs for the associations between diabetes mellitus and density food outlets.
Note: The values show AME from logistic regressions in panels B and C; 95% CIs in brackets; horizontal bars = 95% CIs. Density = the number of each food outlet per total number of food outlets within 300 m of a residents home address. Proximity = 1 if having at least 1 outlet within 100 m of a residents home address and 0 if otherwise. AME, average marginal effect; FFR, fast-food restaurant.
Regarding the associations between the proximity of food outlets and diabetes mellitus, no statistically significant results were found for the share of supermarket, corner stores, stationary carts, and mobile carts (Table 3, panels B and C). However, results showed that the proximity of FFR near home was positively associated with the probability of having high blood glucose level and being diagnosed with diabetes. Having at least 1 FFR near home was associated 16% (odds ratio [OR]: 1.16; CI: 1.01, 1.33; p < 0.05) and 19% (OR: 1.19; CI: 1.03, 1.38; p < 0.05) increases in the odds of having high blood glucose and being diagnosed diabetes, respectively. The association between FFR proximity and having high blood glucose was statistically significant for males (OR: 1.29; CI: 1.03, 1.63; p < 0.05) but not females, although the effect sizes are of similar order of magnitude. Associations of the proximity to FFR and high blood glucose were statistically significant only for high-income earners (OR: 1.37; CI: 1.13, 1.67; p < 0.01). The association between FFR proximity and having a diabetes mellitus diagnosis was statistically significant only in those with higher income (OR: 1.33; CI: 1.08, 1.64; p < 0.01) (Fig 3, Tables 2 and 3).

Fig 3. ORs for the associations between diabetes mellitus and proximity of food outlets.
Note: The values show AORs from logistic regressions in panels B and C; 95% CIs in brackets; horizontal bars = 95% CIs. Density = the number of each food outlet per total number of food outlets within 300 m of a residents home address. Proximity = 1 if having at least 1 outlet within 100 m of a residents home address and 0 if otherwise. AOR, adjusted odds ratio; FFR, fast-food restaurant; OR, odds ratio.
Discussion
We examined the associations of density and proximity of healthy and unhealthy food outlets with T2DM, as well as the heterogeneity of such associations by sex and income in Bangladesh and Sri Lanka. We used a unique dataset that merged individual-level surveillance data (South Asia Biobank) with built environment data measuring individual exposure to healthy and unhealthy food outlets.
We found that the share of FFR was higher in Bangladesh (among the country with the biggest number of people with T2DM in 2019) [1], while the shares of corner stores and supermarkets were higher in Sri Lanka. All supermarkets were identified in urban sites. We identified that T2DM levels were higher among females and higher-income participants.
When testing the association of the food environment and diabetes mellitus, no significant findings were identified in relation to the share of supermarket, corner stores, stationary carts, nor mobile carts. However, an observed key finding of our study was that FFR share, density, and proximity were all associated with a greater risk of T2DM. These findings are consistent with previous evidence from high-income countries such as UK and Sweden where unhealthy food outlets have been found to increase the odds of developing T2DM [4,5].
With regard to sex differences, a higher FFR density was associated with greater blood glucose, higher likelihood of high blood glucose for female but not male, and higher chances of being diagnosed with DM for both female and male. Proximity to FFR was associated with a higher blood glucose level in males but does not seem to play a role in the likelihood of being diagnosed with diabetes for both male and female. These sex differences could be due to differences in exposure metricsdensity and proximitycapturing different dimensions of decision-making for food sourcing. Previous studies have shown differences in how men and women engage differently to the food environment [4]. Therefore, our finding could be explained by how sex affects perception of and interaction with the surrounding environment. With lower labor market participation than men in these countries, women spend more time with household chores including sourcing foods, and, therefore, it is plausible that they get more exposed to a range of outlets around their homes [4], rendering density of outlets more salient in their food choices. Labor market participation of women in Sri Lanka is particularly low in urban environments [22] that tend to be characterized by wider availability of FFRs. With higher labor market participation, men are more time constrained due to employment and thus interact with the environment on more sporadic contexts where proximity and convenience become relevant factors for decision-making [4].
Another possible channel for these associations may be sex differences with regard to overall dietary preferences and habitual dietary intakes. For example, previous studies have shown that women have a higher intake of sugar compared with men. To further unpack these associations, one would need time use survey combined with a mapping of how each individual interacts with the environment (e.g., where they shop, how frequently, and what they buy).
While our data do not enable us to assess these mechanisms, the sex differences on the role of the food environment on diabetes have important public health implications. Because South Asians have a greater visceral adiposity and insulin resistance, impaired -cell function, and a genetic predisposition to diabetes, which culminates in a markedly increased risk that may lead to the development of T2DM [23], they should be targeted for prevention. South Asian women in particular are more likely to have diabetes than white women [24,25]. While the diagnosis of diabetes doubles the cardiovascular risk in men, it more than triples the risk in women. Women are also at greater risk of other diabetes-related complications such as blindness, kidney disease, and depression [24]. Therefore, our results suggest that interventions in the food environments may be particularly important for women in these countries. Examples of interventions include the subsidization of healthy food and taxation of fast food, nutritional labeling in menus in FFRs, and nutritional literacy interventions that discourage the consumption of fast food.
Our findings also showed that T2DM risk variations by income, with exposure (through density and proximity) to FFRs affecting more blood glucose and likelihood of being diagnosed diabetes for high-income earners. These findings are consistent with existing evidence that shows diabetes being more prevalent among the wealthy groups [26]. With rapid shifts in lifestyle characterized by a nutritional transition and urbanization [27], the increased availability and accessibility of unhealthy food, combined with a raise in economic purchasing power, generates greater opportunities to eat out of home, which, with the proliferation of fast-food establishments, may contribute to the formation of unhealthy habitual dietary patterns [28]. In LMICs, western shops selling processed foods and fast-food restaurants strategically locate in higher-income neighborhoods [29] to target those that can afford these foods. These foods also tend to be more expensive than fresh produce and FV. Therefore, these could explain why upper-income populations are more affected by being exposed to more obesogenic environments.
In addition, evidence also suggests that the wealthier tend to shop at conveniently located stores around their neighborhoods, while low-income individuals are more likely to travel long distances to shop at cheaper markets or street stalls [30]. Therefore, it is plausible that exposure to unhealthy environments plays a stronger role in explaining prevalence of diabetes for the wealthier than for those with low income.
These findings highlight the need for public health interventions targeting high-income earners. Given that affordability may not be a key factor for decision-making among high-income earners, diabetes prevention strategies should include improving the saliency and convenience of accessing healthy foods, as well as improving nutritional literacy.
However, preventive strategies are also required to prevent lower-income populations to develop risk factors that may lead T2DM. Indeed, although to a lesser extent than for high-income earners, our results suggest that density of fast foods is positively associated with the likelihood of being diagnosed with diabetes also for low-income earners. Recent evidence on obesity trends, a risk factor of diabetes, shows that as the LMICs gross domestic product (GDP) increases the rates of obesity among low SES group increases with the shift of obesity occurring first in low SES women [31]. Due to financial, educational, mobility, and time constrains, low-income populations may have less opportunities to consume healthy foods [32]. Thus, food environments that are more prone to facilitate unhealthy food choices in combination with the absence of fiscal policies and regulations on access to healthy foods may affect more disproportionally the lower-income groups in the future to come. Therefore, upstream policies guided by a health in all policies approach that explicitly target the key social, economic, and structural determinants of health and behaviors may become essential to prevent diabetes [33]. Such approaches may include unhealthy food and beverage taxation, subsidies for healthy foods, food labeling on menus, banning unhealthy food advertising, as well as promoting better urban planning and subsidized transport that facilitate access to healthy foods and encourage physical activity [33].
To summarize, consistent with other research in South Asia [11], our results suggest interventions targeting the environment may be effective in preventing diabetes; however, the heterogeneity of the associations found in our analysis suggests that more specific interventions may be needed. This is aligned with other evidence indicating that one-size-fits-all built environment interventions have not led to improved outcomes [12], and future research is needed to evaluate which food environment interventions could improve diabetes outcomes in this geographical region and population.
There are at least 5 limitations of our study. First, since we used cross-sectional individual level data, temporality in the associations cannot be established. Second, given the cross-sectional nature of the data, our study is descriptive and does not enable identifying the causal impacts of the environment on the outcomes assessed. While we control for a range of cofounders, we cannot fully address all endogeneity and reverse causality concerns (e.g., unobserved food preferences of those at risk of diabetes may be such that they locate in places with a high density of unhealthy food outlets). Third, we captured only part of the environment with the 300-m buffer. Even though this is commonly used in the literature to examine built environment and health behavior/outcomes [18,19], this approach implies that we may imperfectly capture exposure to obesogenic food environments as we do not measure whether participations shop beyond the assessed areas. To investigate those effects in a meaningful way would require an understanding of where individuals gravitate beyond their residential neighborhoods to infer their individual level exposure to different food environments. Despite this limitation, focusing on a narrow definition of the built environments around homes has the advantage of considering outlets in areas where individuals are highly likely to gravitate to during the day and are, therefore, likely to use. Importantly, some of the drawbacks of considering small buffers in countries where food outlets are clustered in different parts of towns (e.g. large supermarkets outside of the city center, while fast food outlets in commercial and business areas), are mitigated in the geographies we assess, where there is an abundance of a variety of food outlets in the immediacies of individuals homes. Fourth, we measured food environments using residency geolocation; however, participants may consume part of their meals far from home (e.g., if the workplace is distant). Also, we measured exposure based on residency rather than relying on individual shopping data and consumption patterns. Such data are not available, although it could be important to further identify the heterogeneity of the observed associations. Fifth, we categorized the extent to which food environments are healthy and unhealthy based on the international classification in the absence of a classification for South Asian countries. Since we did not observe food sold in these food outlets and lacked consumption data, the magnitude of the associations may reflect the mix of healthy and unhealthy foods available in these outlets in particular supermarkets. Despite these caveats, our study provides novel evidence on the association between food environment and T2DM as well as its unequal associations by sex and income.
References
- 1.
International Diabetes Federation (IDF). IDF Diabetes Atlas, 9th ed. 2019. Available from: https://diabetesatlas.org/en. - 2.
World Health Organization (WHO). Global Report on Diabetes. 2016. Available from: https://www.who.int/publications/i/item/9789241565257. pmid:26558682 - 3.
Chan JCN, Lim L-L, Wareham NJ, Shaw JE, Orchard TJ, Zhang P, et al. The Lancet Commission on diabetes: using data to transform diabetes care and patient lives. Lancet. 2020;396:201982. pmid:33189186 - 4.
Sarkar C, Webster C, Gallacher J. Are exposures to ready-to-eat food environments associated with type 2 diabetes? A cross-sectional study of 347 551 UK Biobank adult participants. Lancet Planet Health. 2018;2:e43850. pmid:30318101 - 5.
Mezuk B, Li X, Cederin K, Rice K, Sundquist J, Sundquist K. Beyond Access: Characteristics of the Food Environment and Risk of Diabetes. Am J Epidemiol. 2016;183:112937. pmid:27240801 - 6.
den Braver NR, Lakerveld J, Rutters F, Schoonmade LJ, Brug J, Beulens JWJ. Built environmental characteristics and diabetes: a systematic review and meta-analysis. BMC Med. 2018;16:126. pmid:29382337 - 7.
IDF. Southeast Asia Members. 2020. Available from: https://idf.org/our-network/regions-members/south-east-asia/members.html. - 8.
World Obesity Federation (WOF). World Obesity Federation Global Obesity Observatory. 2021. Available from: https://data.worldobesity.org. - 9.
Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP. Food consumption of Sri Lankan adults: an appraisal of serving characteristics. Public Health Nutr. 2013;16:6538. pmid:22784794 - 10.
Bhowmik S. Street vendors in Asia: a review. Econ Polit Wkly. 2005;40:225664. - 11.
Atanasova P, Kusuma D, Pineda E, Anjana RM, De Silva L, Hanif AAM, et al. Food environments and obesity: A geospatial analysis of the South Asia Biobank, income and sex inequalities. SSM Popul Health. 2022;17:101055. pmid:35252534 - 12.
Atanasova P, Frost G, Miraldo M, et al. The impact of the consumer and neighbourhood food environment on dietary intake and obesity: A systematic review of causal impact studies. Soc Sci Med. 2022;299:114879. pmid:35290815 - 13.
Song P, Gupta A, Goon IY, Hasan M, Mahmood S, Pradeepa R, et al. Data Resource Profile: Understanding the patterns and determinants of health in South Asiansthe South Asia Biobank. Int J Epidemiol. 2021;50:717718e. pmid:34143882 - 14.
Dez J, Cebrecos A, Galn I, Prez-Freixo H, Franco M, Bilal U. Assessing the Retail Food Environment in Madrid: An Evaluation of Administrative Data against Ground Truthing. Int J Environ Res Public Health. 2019;16:3538. pmid:31546670 - 15.
Babey SH, Diamant AL, Hastert TA, Harold G. UCLA Recent Work Title Designed for Disease: The Link Between Local Food Environments and Obesity and Diabetes. 2008. Available from: https://escholarship.org/uc/item/7sf9t5wx. - 16.
North American Industry Classification System (NAICS) U.S. Census Bureau. Available from: https://www.census.gov/naics. - 17.
Public Health Advocates (PHA). Designed for Disease The Link Between Local Food Environments and Obesity and Diabetes. Available from: www.publichealthadvocacy.org/research. - 18.
Duncan DT, Kawachi I, Subramanian SV, Aldstadt J, Melly SJ, Williams DR. Examination of How Neighborhood Definition Influences Measurements of Youths Access to Tobacco Retailers: A Methodological Note on Spatial Misclassification. Am J Epidemiol. 2014;179:373. pmid:24148710 - 19.
Bodor JN, Rose D, Farley TA, Swalm C, Scott SK. Neighbourhood fruit and vegetable availability and consumption: the role of small food stores in an urban environment. Public Health Nutr. 2008;11:41320. pmid:17617930 - 20.
Baker J, White N, Mengersen K. Spatial modelling of type II diabetes outcomes: a systematic review of approaches used. R Soc Open Sci. 2014;2. pmid:26543572 - 21.
Wichaidit W, Sangthong R, Chongsuvivatwong V, McNeil E, Chariyalertsak S, Kessomboon P, et al. Religious affiliation and disparities in risk of non-communicable diseases and health behaviours: Findings from the fourth Thai National Health Examination Survey. Glob Public Health. 2014;9:42635. pmid:24684694 - 22.
Solotaroff JL, Joseph G, Kuriakose AT, Sethi J. Getting to Work Unlocking Womens Potential in Sri Lankas Labor Force. Washington DC: World Bank; 2020. - 23.
Shah A, Kanaya AM. Diabetes and Associated Complications in the South Asian Population. Curr Cardiol Rep. 2014;16:116. pmid:24643902 - 24.
Kautzky-Willer A, Harreiter J, Pacini G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr Rev. 2016;37:278316. pmid:27159875 - 25.
Bower JK, Butler BN, Bose-Brill S, Kue J, Wassel CL. Racial/Ethnic Differences in Diabetes Screening and Hyperglycemia Among US Women After Gestational Diabetes. Prev Chronic Dis. 2019;16. pmid:31651379 - 26.
Dagenais GR, Gerstein HC, Zhang X, McQueen M, Lear S, Lopez-Jaramillo P, et al. Variations in Diabetes Prevalence in Low-, Middle-, and High-Income Countries: Results From the Prospective Urban and Rural Epidemiological Study. Diabetes Care. 2016;39:7807. pmid:26965719 - 27.
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70:321. pmid:22221213 - 28.
Diabetes UK. The risk factors of type 2 diabetes. Available from: https://www.diabetes.org.uk/preventing-type-2-diabetes/diabetes-risk-factors. - 29.
Hawkes C. Dietary Implications of Supermarket Development: A Global Perspective. Dev Policy Rev. 2008;26:65792. - 30.
Seidler E. Proceedings of the regional seminar Food into Cities. Collection AC/37-01E. 2001. - 31.
Templin T, Hashiguchi TCO, Thomson B, Dieleman J, Bendavid E. The overweight and obesity transition from the wealthy to the poor in low- and middle-income countries: A survey of household data from 103 countries. PLoS Med. 2019;16:e1002968. pmid:31774821 - 32.
Farrell P, Thow AM, Abimbola S, Faruqui N, Negin J. How food insecurity could lead to obesity in LMICsWhen not enough is too much: a realist review of how food insecurity could lead to obesity in low- and middle-income countries. Health Promot Int. 2018;33:81226. pmid:28541498 - 33.
Swinburn B, Sacks G, Vandevijvere S, Kumanyika S, Lobstein T, Neal B, et al. INFORMAS (International Network for Food and Obesity/non-communicable diseases Research, Monitoring and Action Support): Overview and key principles. Obes Rev. 2013;14:112.